Decoding Beck's Triad: Cardiac Tamponade for EMTs
Master Beck's Triad for the NREMT. Learn the pathophysiology of cardiac tamponade, how to identify the three classic clinical signs, and key field treatments.
· 14 min read
Read →
Master the Rule of Nines for the NREMT. Learn burn classifications, adult vs. pediatric calculations, fluid resuscitation formulas, and critical field care.
When you respond to a burn emergency, your assessment must be swift, structured, and clinically precise. Burn injuries are visually shocking, but you cannot let the dramatic appearance of charred skin distract you from systemic priorities. You need to establish the patient’s airway, verify adequate breathing, manage circulation, and quickly estimate the size and severity of the burn. This estimation determines not only the initial volume of intravenous fluids the patient will receive but also whether they require direct transport to a regional burn specialty center.
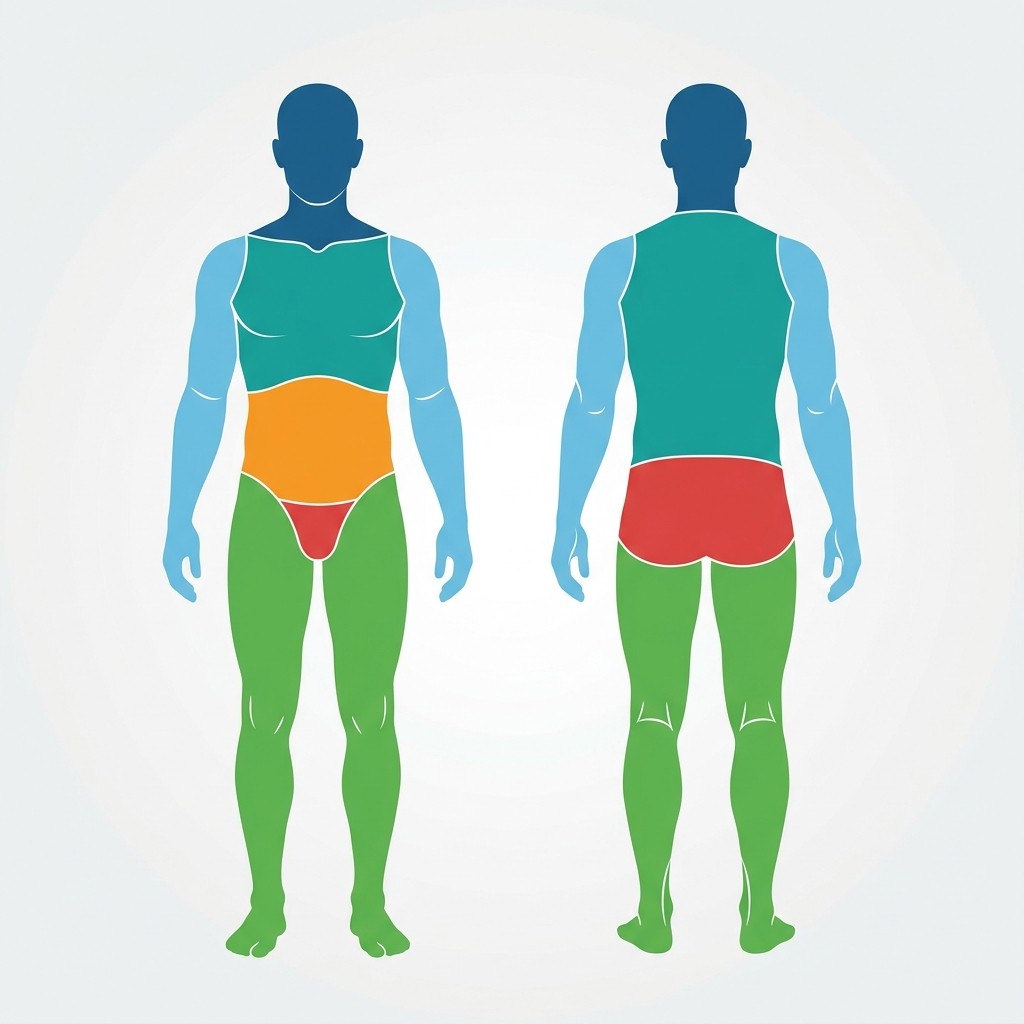
To make these calculations in high-pressure field environments, emergency medical professionals rely on the Rule of Nines. By dividing the human body into specific regions representing nine percent (or multiples of nine percent) of the total surface area, this system provides a rapid, reliable mental calculator.
Let’s unpack how the Rule of Nines works, how it adapts for pediatric patients, and how you apply it to pass the NREMT and save lives in the field.
The human body changes proportions as it grows. Because of these developmental differences, you cannot use the adult body proportions to calculate burn surface area on an infant or child. Doing so will result in dangerous medication or fluid dosing errors.
In infants and toddlers, the head is much larger relative to the rest of the body, while the lower extremities are significantly smaller. As children mature, these ratios shift. The head occupies a smaller percentage of the total surface area, and the legs grow to assume their full adult proportions.
The table below outlines the regional percentages for adults, children, and infants. Memorizing these distinct values is a critical step to pass the NREMT exam.
| Anatomical Region | Adult Percentage | Child (Ages 1 to 8) | Infant (Under Age 1) |
|---|---|---|---|
| Head (Entire Front & Back) | 9% | 12% | 18% |
| Anterior Torso (Chest & Abdomen) | 18% | 18% | 18% |
| Posterior Torso (Back & Buttocks) | 18% | 18% | 18% |
| Each Arm (Entire Left or Right) | 9% | 9% | 9% |
| Each Leg (Entire Left or Right) | 18% | 16.5% | 14% |
| Perineum (Genitalia) | 1% | 1% | 1% |
| Total Body Surface Area | 100% | 100% | 100% |
For smaller, scattered, or irregular burns, the Rule of Nines can become clunky. In these situations, you should apply the Palmar Method.
This technique uses the patient’s own hand as a template. The surface area of the patient’s palm, including their fingers, represents approximately 1% of their total body surface area. You can mentally overlay the size of the patient’s hand onto the burned areas to estimate the total TBSA. Always use the patient’s hand size, not your own, to make this estimation.
Before you begin calculating TBSA, you must understand which burns to include in your calculations. Burns are classified by the depth of tissue damage. You must exclude superficial burns from your total TBSA calculation.
Superficial burns involve only the epidermis, which is the outermost layer of the skin. A classic example is a mild sunburn. The skin appears red, warm, and dry, and it is tender to the touch. There are no blisters.
Superficial burns do not disrupt the skin’s fluid barrier. Because they do not cause significant fluid shifts or place the patient at risk for systemic shock, you must exclude them from your Rule of Nines calculations.
Partial-thickness burns penetrate through the epidermis and damage the dermis, which is the deeper layer containing blood vessels, nerves, hair follicles, and sweat glands. These burns are characterized by intense pain, deep redness, and clear blisters. The skin may appear moist or wet due to leaking plasma.
Because the dermal layer is compromised, these burns cause significant fluid loss. You must include all partial-thickness burns in your Rule of Nines calculations.
Full-thickness burns destroy the epidermis and the entire dermis, extending into the subcutaneous fat, muscle, or bone beneath. The skin may appear charred, white, leathery, or waxy. Because the sensory nerve endings are completely destroyed, the burn area itself is typically painless, though surrounding partial-thickness areas will remain extremely painful.
Full-thickness burns destroy the skin’s primary protective barriers, leaving the patient highly susceptible to severe infection, hypothermia, and hypovolemic shock. You must include all full-thickness burns in your calculations.
To calculate TBSA, you must assess the patient systematically. Divide the body into its anatomical regions, determine the depth of the burn in each region, and add the percentages of the qualifying areas together.
An adult’s body is divided into simple portions of 9%:
Imagine you are treating a 22-year-old male with blistering burns on his entire chest, his entire abdomen, and the front of his left arm. How would you calculate the TBSA?
Children have different head-to-body ratios. For an infant under one year of age:
For older children (ages 1 to 8), you should adjust the head down and the legs up. A good rule of thumb is to subtract 1% from the head for each year of age over one, and distribute that percentage equally to the legs until the child reaches adult proportions.
Your treatment for burn patients must focus on stopping the burning process, supporting respiration, maintaining body temperature, and preventing shock for EMTs.
Always look for signs of airway burns. Inhalation injuries can cause rapid, life-threatening airway swelling. Watch for:
If you suspect inhalation injury, administer high-flow oxygen immediately using a non-rebreather mask and prepare for rapid transport. If the airway swells shut, securing it becomes exceptionally difficult.
Cool small burns (less than 10% TBSA) using clean, cool water or saline for less than 60 seconds. Do not apply ice, as extreme cold constricts blood vessels and worsens tissue damage. For larger burns, do not apply wet dressings, as this can cause rapid heat loss and trigger severe hypothermia. Cover large burns with dry, sterile, non-adherent dressings or clean dry sheets.
Always remove the patient’s clothing and jewelry. Fabric can retain heat, and metal rings or watch bands will act as tourniquets when the limbs begin to swell. If clothing is melted and stuck to the burn, cut around it. Do not pull adhered fabric away from damaged skin.
Large burns disrupt systemic vascular permeability, causing massive fluid shifts from the blood vessels into the surrounding tissues. This fluid shift leads to severe burn shock. Advanced providers use the Parkland Formula to calculate the volume of intravenous crystalloid fluids (typically Lactated Ringer’s) needed to maintain perfusion.
The formula is structured as follows:
The total calculated volume is administered over a 24-hour period:
Understanding how to calculate these volumes during a patient assessment is a key skill for advanced prehospital providers.
Use this interactive quiz to test your comprehension of TBSA calculations, burn classifications, and emergency resuscitation protocols.
You are treating a 34-year-old female who was pulled from a house fire. She presents with blistering burns across her entire anterior chest and abdomen, as well as the entire surface of her left arm. What is the estimated Total Body Surface Area (TBSA) burned?
Filed Under
About the Author
Veteran EMT with 13+ years of field experience in EMS. I built EMT Training Station to give aspiring first responders the honest, practical information I wish I'd had when starting out — covering training, certification, gear, and career advancement.
Master Beck's Triad for the NREMT. Learn the pathophysiology of cardiac tamponade, how to identify the three classic clinical signs, and key field treatments.
Learn how to write professional patient care report (PCR) narratives that protect your EMS career. Master SOAP vs CHART models and document critical negatives.
Learn how to recognize Cushing's Triad in the field, understand the Monro-Kellie doctrine, and differentiate increased intracranial pressure from systemic shock.