How to Become a Flight Paramedic: The Complete Career Track
Learn how to become a flight paramedic. Read this step-by-step career roadmap covering clinical requirements, critical care certifications, and physical standards.
· 8 min read
Read →
Shock is not just low blood pressure — it is a systemic cellular crisis. This EMS field guide breaks down the four types of shock, the stages of compensation, capnography as a perfusion tool, and BLS priorities for managing a crashing patient.
Every EMT student learns the textbook definition of shock. They memorize the phrase “inadequate tissue perfusion” and move on to the next chapter. But when you are standing in the field, shock does not look like a vocabulary definition. It looks like a clock ticking down.
To truly understand shock, you have to look past the blood pressure cuff. You must learn to see what is happening at the microscopic level. Shock is not just low blood pressure. It is a systemic cellular crisis. When cells are starved of oxygen and nutrients, they switch from clean energy production to a dirty, toxic survival mode. If you do not intervene quickly, that cellular damage cascades until the entire system fails.
This guide strips away the clinical fluff. We will break down the underlying mechanics of shock, explore the four primary categories you will encounter on the street, look at advanced diagnostic tools like capnography, and evaluate how to spot the subtle signs of compensation before it is too late. For a broader look at how the heart and vasculature function under normal conditions, review our cardiovascular system for EMTs guide.
To keep a human body alive, the cardiovascular system relies on a perfectly balanced plumbing network. This network requires three intact components: a functional pump, a specific volume of fluid, and a sealed system of pipes. If any single one of these components fails, the entire system loses pressure. Perfusion stops.
When you encounter a patient in shock, your first diagnostic task is determining which part of the plumbing broke. The global EMS community classifies these failures into four primary buckets.
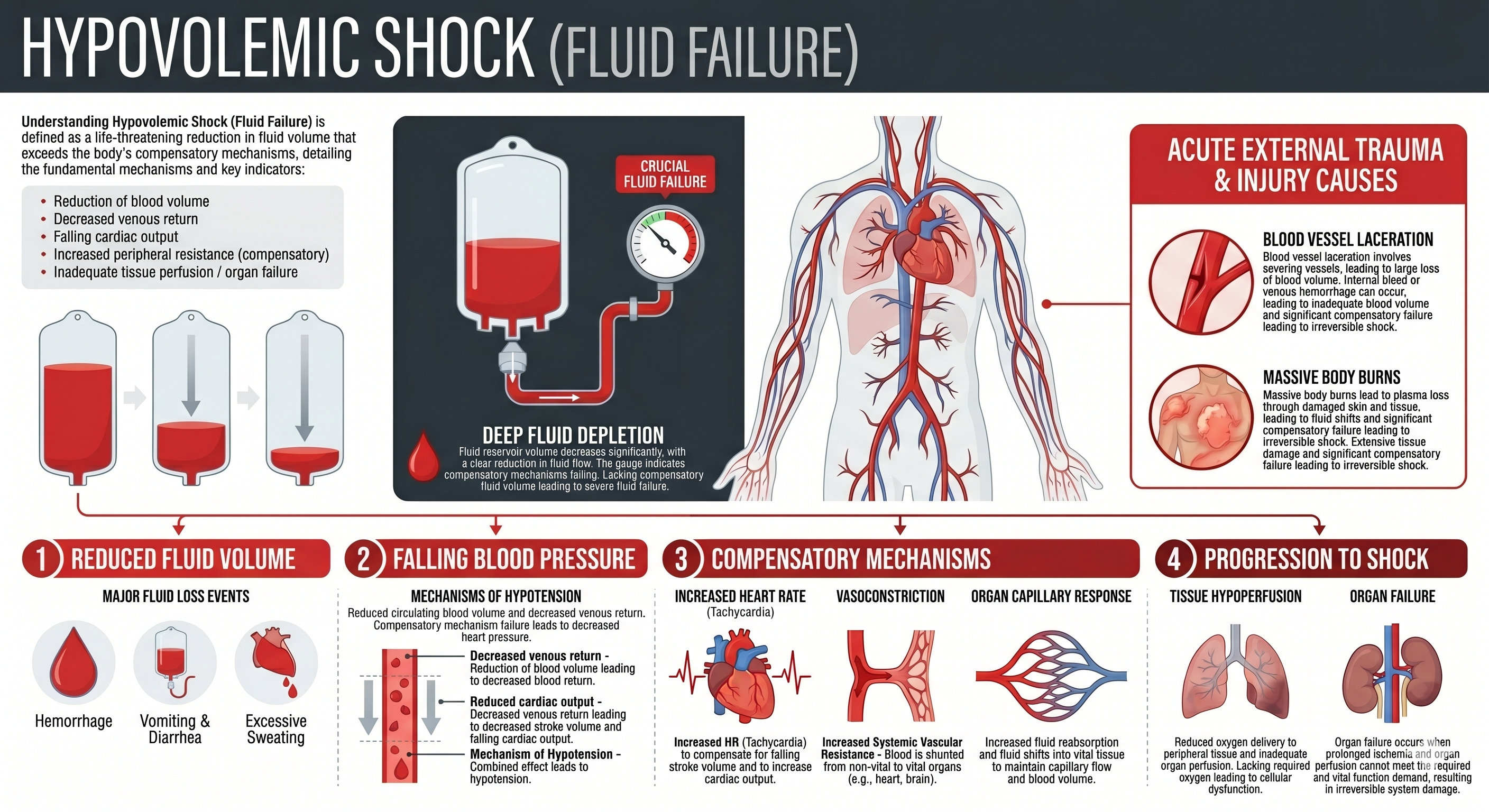
This is the most straightforward type of shock. The plumbing system simply lacks enough fluid to completely fill the pipes. This can happen through direct, catastrophic blood loss from a traumatic laceration. It can also happen through severe dehydration, protracted vomiting, or massive burns. Without enough fluid volume, the heart cannot generate enough pressure to push oxygen to the brain.
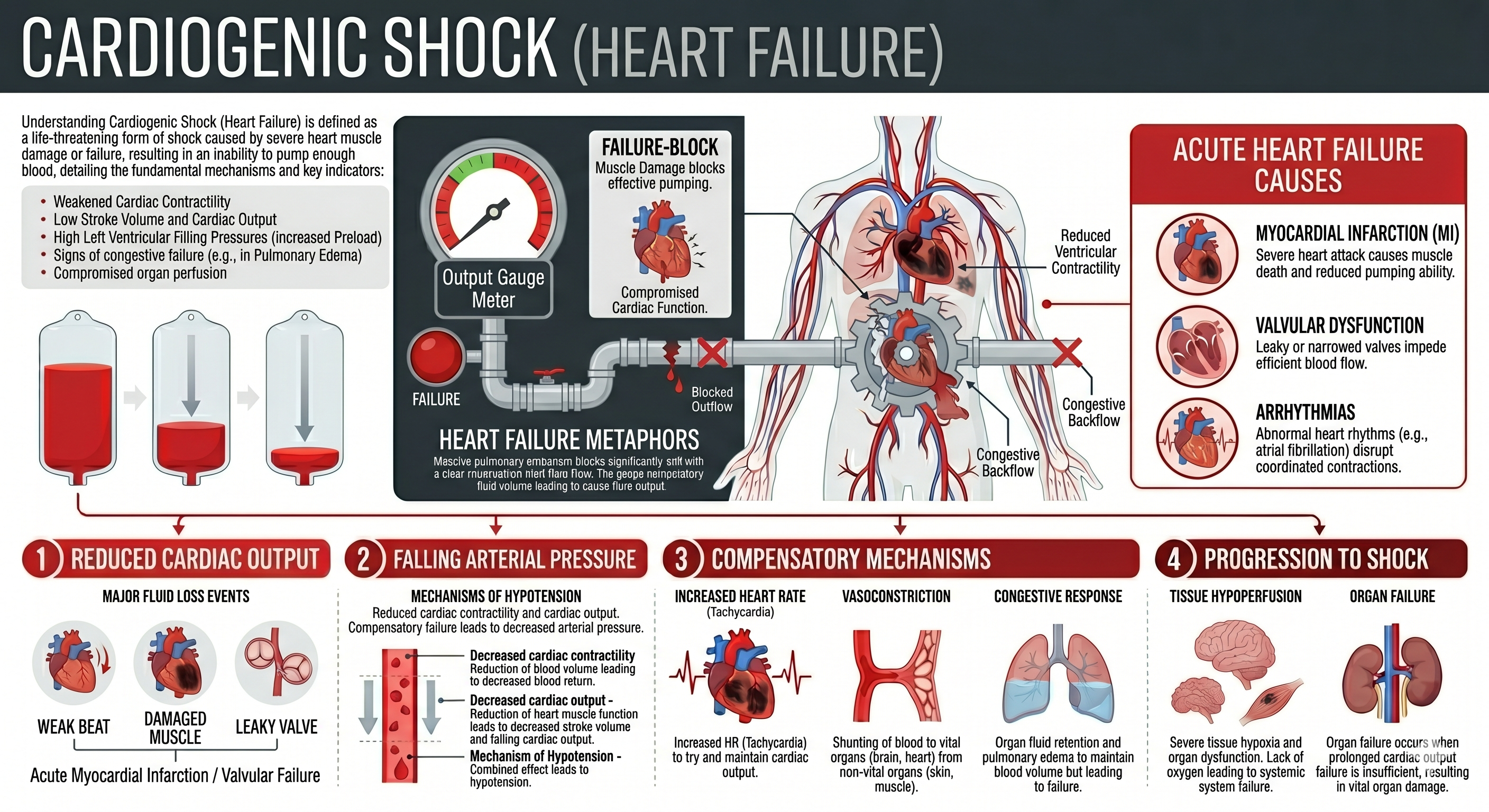
In this scenario, the fluid volume is perfectly fine and the pipes are intact. The problem lies entirely within the pump itself. The heart muscle has suffered significant damage, often from a massive myocardial infarction. Because the muscle is bruised or dying, it can no longer squeeze with enough structural force to circulate blood effectively. For a deeper look at the cardiac conditions that lead here, see our guide on the cardiovascular system for EMTs.
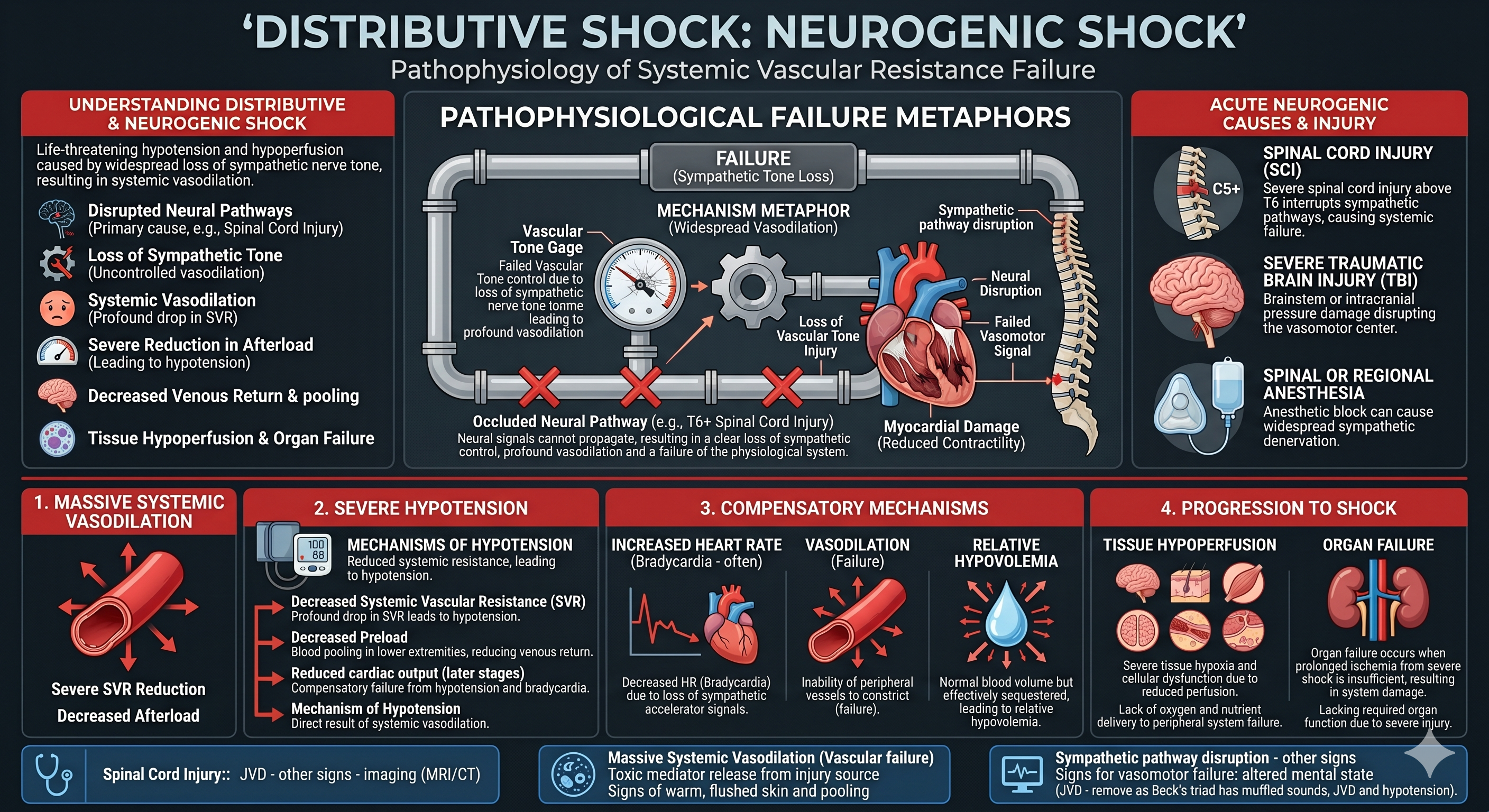
This type of shock is often the hardest for new students to visualize. The fluid volume is normal, and the heart is pumping well. However, the pipes have suddenly dilated to twice their normal size. This massive, widespread vasodilation happens during severe allergic anaphylaxis, overwhelming systemic sepsis, or neurogenic spinal cord injuries. Because the container has suddenly grown much larger than the liquid inside it, the systemic blood pressure plummets instantly.
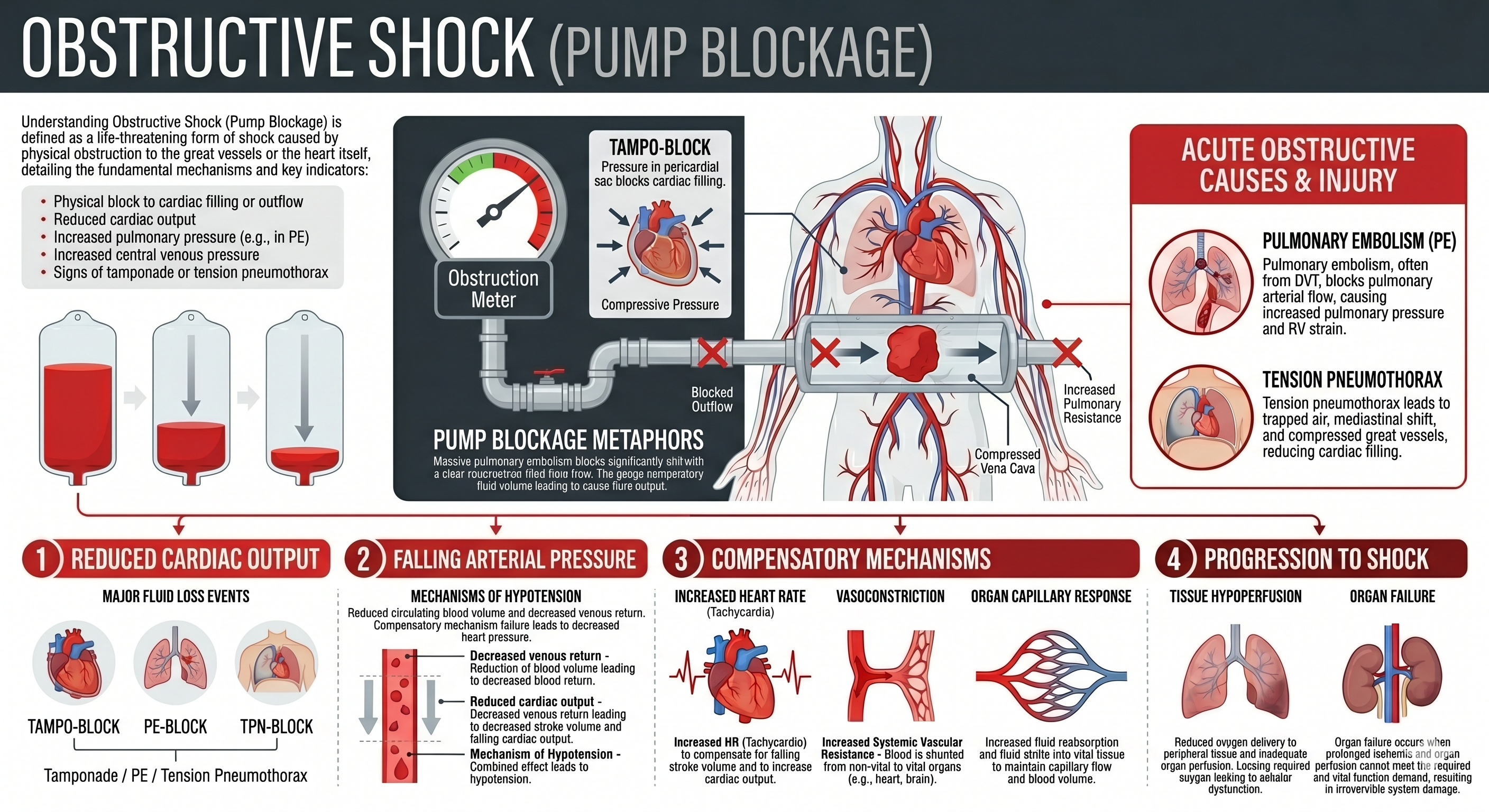
The pump is fine, the fluid is full, and the pipes are normal. But a physical obstacle is preventing the fluid from moving through the circuit. A massive pulmonary embolism can block the blood flow to the lungs. A tension pneumothorax can shift the structures of the chest, physically compressing the vena cava and preventing blood from returning to the heart. Another classic cause of obstructive shock is cardiac tamponade, which presents with the physical findings of Beck’s Triad.
The biggest mistake a rookie provider can make is waiting for a low blood pressure reading to diagnose shock. Hypotension is not an early warning sign. It is a terminal drop. The human body is incredibly resilient, and it will fight aggressively to maintain homeostatic balance using two distinct operational phases.
During this initial phase, the body recognizes that pressure is dropping and immediately sounds the alarm. The sympathetic nervous system kicks into overdrive. It floods the bloodstream with epinephrine. The heart rate accelerates to push blood faster. The peripheral blood vessels constrict sharply, shunting blood away from non-essential zones like the skin and digestive tract to preserve the brain and kidneys.
What you will see: The patient will be anxious, restless, or slightly confused as the brain senses early oxygen deprivation. Their skin will become pale, cool, and clammy as blood shunts inward. Their heart rate and respiratory rate will elevate.
When performing your patient history and assessment, pay close attention to the subjective complaint. A patient who says they feel “weird,” dizzy, or unusually anxious after a trauma mechanism or allergic exposure should trigger your shock index immediately — regardless of what the blood pressure reads.
Eventually, the body runs out of resources. The cellular mechanisms can no longer keep up with the overwhelming deficit. The compensatory measures fail, and the system begins to slide backward down the mountain.
What you will see: This is the phase where the blood pressure finally drops. The patient will display profound hypotension. Their mental status will deteriorate from anxious confusion to lethargy or complete unconsciousness. Their pulses will become weak, thready, or entirely absent at the radial artery.
Early altered mental status is the most reliable indicator you have. A focused neurological assessment — checking orientation, pupillary response, and motor response — should be a standard component of every shock workup.
For decades, EMS systems used end-tidal carbon dioxide monitoring, known as EtCO₂, solely to verify that an endotracheal tube was placed correctly in the trachea. Today, we know that continuous waveform capnography is actually a powerful window into systemic perfusion and metabolic health. It is a multi-purpose tool that tracks your patient’s circulatory status in real time.
Exhaled carbon dioxide levels rely directly on three physiological factors: cellular metabolism, clear airways, and adequate blood flow to the lungs. If a patient is breathing at a steady rate, their EtCO₂ reading reflects their cardiac output.
A normal adult EtCO₂ reading falls between 35 and 45 mmHg. When a patient enters a shock state, their organs suffer from hypoperfusion, and systemic metabolism drops. Because less blood is circulating back to the right side of the heart, less carbon dioxide is delivered to the lungs for elimination. This causes the EtCO₂ number on your monitor to drop, even if the patient’s breathing rate looks completely normal.
| EtCO₂ Reading | Clinical Interpretation | Immediate Action Needed |
|---|---|---|
| 35–45 mmHg | Normal metabolic and perfusion status | Monitor trends and support baseline ABCs |
| 30–34 mmHg | Early hypoperfusion or mild metabolic distress | Reassess skin vitals, prepare IV access, check fluids |
| Below 25 mmHg | Critical indicator of hemorrhagic or septic shock | Initiate high-priority transport, aggressive fluid or blood resuscitation |
| 12 mmHg or lower | Imminent cardiopulmonary collapse | Extreme danger zone — maximum mortality risk, adjust treatment immediately |
Utilizing capnography allows you to catch hidden hypoperfusion early, adjust your clinical treatment plans, and provide an accurate radio alert to the receiving trauma center.
When managing a patient in shock, you cannot fix the underlying pathology in the back of the rig. You cannot repair a damaged heart muscle or cure a systemic bacterial infection on the street. Your goal is stabilization and rapid transport to definitive care. Field management relies on an aggressive, unyielding focus on basic life support fundamentals.
Secure the Airway and Oxygenate: High-flow oxygen is a non-negotiable baseline for shock management. If the red blood cells are scarce or moving slowly, every single cell must be fully saturated with oxygen. Ensure the airway is patent and assist ventilations with a bag-valve-mask if the respiratory drive begins to fail.
Preserve Body Temperature: Hypothermia is a silent killer in shock patients. When a body becomes cold, it loses its ability to clot blood effectively, accelerating internal hemorrhaging. Strip away wet clothing immediately. Cover the patient with warm blankets, and keep the patient compartment of your ambulance uncomfortably hot.
Position for Success: Place the patient in a supine position to maximize blood flow to the core organs. Avoid the outdated trend of aggressively elevating the legs, as this can compress abdominal organs against the diaphragm and compromise breathing. Keep them flat, warm, and secure.
The most reliable early sign of shock is altered mental status, which often presents as unexplained anxiety, restlessness, or combativeness. This happens because the brain senses micro-fluctuations in oxygenation before peripheral physical vital signs change. Cool, pale, and clammy skin is another excellent early indicator that the body is shunting blood to its core.
Low blood pressure is a late sign because the human body uses powerful mechanisms, including a fast heart rate and systemic vasoconstriction, to keep the plumbing system pressurized. A drop in systolic blood pressure means these compensatory resources are completely exhausted, signaling that the patient is sliding into decompensated shock.
Capnography measures the carbon dioxide exhaled from the lungs, which relies entirely on adequate blood flow returning from the body. In a shock state, poor systemic perfusion means less blood reaches the lungs, causing the EtCO₂ reading to drop below 35 mmHg even if the respiratory rate is perfectly normal.
Hypovolemic shock is caused by a structural lack of fluid within the cardiovascular system, such as external bleeding or severe dehydration. Distributive shock occurs when the fluid volume is normal but the blood vessels dilate abnormally wide, making the container too large for the liquid inside.
Shock disrupts the body’s normal temperature regulation, and hypothermia actively interferes with the chemical cascade required for blood clotting. Keeping the patient warm prevents the development of the trauma triad of death, which includes hypothermia, coagulopathy, and acidosis.
The four primary types are hypovolemic (not enough fluid), cardiogenic (pump failure), distributive (vasodilation making the vascular container too large), and obstructive (a physical blockage such as a tension pneumothorax or pulmonary embolism preventing normal circulation). Mastering patient assessment is the key to differentiating them quickly in the field.
Test your understanding of the stages of shock, perfusion physics, capnography, and prehospital shock management with this interactive 5-question NREMT-style quiz.
You are dispatched to a patient who has been vomiting blood. The patient is anxious, has cool, pale, clammy skin, a heart rate of 124, a respiratory rate of 22, and a blood pressure of 102/82. What stage of shock is this patient experiencing?
Filed Under
About the Author
Veteran EMT with 13+ years of field experience in EMS. I built EMT Training Station to give aspiring first responders the honest, practical information I wish I'd had when starting out — covering training, certification, gear, and career advancement.
Learn how to become a flight paramedic. Read this step-by-step career roadmap covering clinical requirements, critical care certifications, and physical standards.
A veteran responder's guide to writing an EMS resume and passing the oral interview. Includes resume templates, certification checklists, and practice questions.
Learn how to become a firefighter EMT. Read this step-by-step career track guide covering EMT certification, CPAT fitness testing, and fire academy prep.