Obstetrics and gynecology (OB/GYN) emergencies represent some of the most high-anxiety calls you will face in prehospital care. Because childbirth is a natural physiological process, the majority of deliveries go smoothly. However, when complications arise, they require rapid recognition and immediate field management.
For the NREMT cognitive exam, you must master the physiological changes of pregnancy, the three distinct stages of labor, the APGAR scoring system, and the management of critical childbirth emergencies.
The Three Stages of Labor
Understanding the stages of labor helps you determine whether to prepare for an on-scene delivery or initiate immediate transport.
Stage 1 (Dilation Stage):
Begins: The onset of regular uterine contractions and thinning (effacement) of the cervix.
Ends: Full dilation of the cervix (10 cm).
Note: This is typically the longest stage, especially for first-time mothers (primigravida). If the amniotic sac ruptures (water breaks), document the time and color of the fluid.
Stage 2 (Expulsion Stage):
Begins: Full cervical dilation and the crowning of the baby’s head.
Ends: Complete delivery of the newborn.
Note: This is the stage where active delivery occurs. If you see crowning, prepare for delivery on scene. Do not attempt to delay delivery.
Stage 3 (Placental Stage):
Begins: Immediately after the newborn is delivered.
Ends: Delivery of the placenta.
Note: The placenta typically delivers within 5 to 30 minutes. Do not pull on the umbilical cord to speed up this process, as this can cause uterine inversion.
Calculating the APGAR Score
The APGAR score is a standardized assessment tool used to evaluate a newborn’s physical condition and transition to extrauterine life. You must calculate the score at 1 minute and 5 minutes post-delivery.
The APGAR mnemonic represents five parameters: Appearance, Pulse, Grimace, Activity, and Respiration. Each category is scored 0, 1, or 2 points.
Parameter
0 Points
1 Point
2 Points
Appearance (Color)
Blue or pale all over
Pink body, blue extremities (acrocyanosis)
Completely pink
Pulse (Heart Rate)
Absent
Slow (less than 100 bpm)
Rapid (over 100 bpm)
Grimace (Irritability)
No response to stimulation
Grimace or weak cry
Vigorous cry, sneeze, or cough
Activity (Muscle Tone)
Limp, flaccid
Some flexion of extremities
Active motion, well-flexed
Respiration (Effort)
Absent
Slow, irregular, weak cry
Strong, lusty cry
Scoring Clinical Decisions
8 to 10 points: Normal, healthy newborn. Keep the baby warm, dry, and initiate skin-to-skin contact.
4 to 7 points: Mild to moderate distress. Rub the baby’s back or flick the soles of the feet to stimulate breathing. Administer blow-by oxygen if necessary.
0 to 3 points: Severe distress. Initiate immediate neonatal resuscitation.
Pre-Delivery Complications
1. Preeclampsia and Eclampsia
Preeclampsia is a pregnancy-induced hypertensive disorder that typically develops after the 20th week of gestation.
Signs and Symptoms: High blood pressure (systolic > 140 mmHg), severe swelling (edema) in the hands and face, persistent headache, and visual disturbances.
Transition to Eclampsia: The disorder escalates to eclampsia when the patient experiences generalized tonic-clonic seizures.
EMT Management: Keep the patient calm, minimize sensory stimulation (dim lights, quiet ride), administer high-flow oxygen, and transport the patient on their left side to prevent supine hypotensive syndrome.
2. Placenta Previa vs. Abruptio Placentae
These represent two major causes of third-trimester bleeding. The NREMT frequently tests your ability to differentiate them.
Placenta Previa: The placenta develops abnormally, covering all or part of the cervical opening.
Clinical Presentation: Painless, bright red vaginal bleeding. The uterus remains soft and non-tender.
Abruptio Placentae: The premature separation of a normally implanted placenta from the uterine wall.
Clinical Presentation: Sudden, severe abdominal pain, rigid or board-like uterus, and variable vaginal bleeding (bleeding can be concealed behind the placenta).
Delivery Complications and Field Protocols
1. Nuchal Cord
A nuchal cord occurs when the umbilical cord wraps around the baby’s neck during delivery.
EMT Protocol: As the head delivers, slip your index finger around the neck to check for the cord. If present, gently slip it over the baby’s head. If the cord is wrapped too tightly to remove, clamp it in two places, cut it between the clamps, and proceed with the delivery immediately.
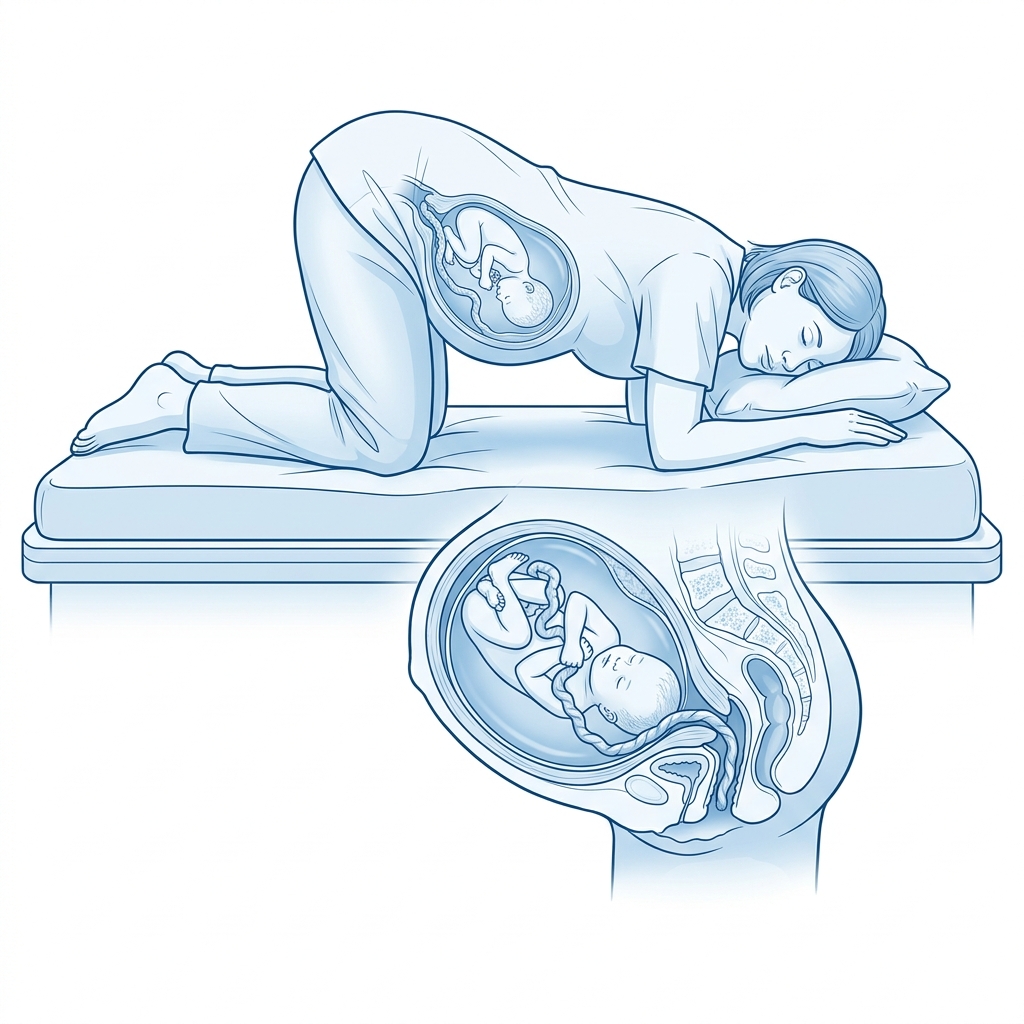
2. Prolapsed Umbilical Cord
A prolapsed cord occurs when the umbilical cord delivers before the baby’s head, causing the head to compress the cord in the birth canal, cutting off the baby’s oxygen supply.
EMT Protocol: This is a true, life-threatening emergency.
Position the mother in a knee-chest or Trendelenburg position to let gravity relieve pressure.
Insert a sterile, gloved hand into the vagina and apply gentle upward pressure on the baby’s head to lift it off the cord. Do not remove your hand until you reach the hospital.
Cover the exposed cord with sterile dressings moistened with warm saline.
Initiate immediate transport.
3. Breech and Limb Presentations
Breech Presentation: The baby delivers buttocks or feet first.
EMT Protocol: If delivery is imminent, support the body as it delivers. To prevent head entrapment, insert two gloved fingers into the vagina to form a “V” shape around the baby’s nose and mouth, creating a small airway space. Transport immediately.
Limb Presentation: A single arm or leg protrudes from the vagina.
EMT Protocol: Delivery cannot occur in the field. Position the mother in a knee-chest position, apply high-flow oxygen, and transport immediately. Never pull on the limb or insert your hand.
Knowledge Check: OB/GYN Practice Quiz
Test your prehospital obstetrics knowledge with this quick check.
NREMT OB/GYN Practice Quiz
Question 1 of 3
During delivery in the field, you notice that the baby's head has delivered, but the umbilical cord is wrapped tightly around the baby's neck. What is your first immediate action?
Veteran EMT with 13+ years of field experience in EMS. I built EMT Training Station to give
aspiring first responders the honest, practical information I wish I'd had when
starting out — covering training, certification, gear, and career advancement.
Master Beck's Triad for the NREMT. Learn the pathophysiology of cardiac tamponade, how to identify the three classic clinical signs, and key field treatments.
Master the Rule of Nines for the NREMT. Learn burn classifications, adult vs. pediatric calculations, fluid resuscitation formulas, and critical field care.
Learn how to write professional patient care report (PCR) narratives that protect your EMS career. Master SOAP vs CHART models and document critical negatives.