How to Become a Flight Paramedic: The Complete Career Track
Learn how to become a flight paramedic. Read this step-by-step career roadmap covering clinical requirements, critical care certifications, and physical standards.
· 8 min read
Read →
Learn the 8 essential lung sounds every EMT and paramedic must recognize — normal, absent, diminished, wheezing, rhonchi, crackles, pleural rub, and stridor — with YouTube audio examples for each.
Updated for 2026
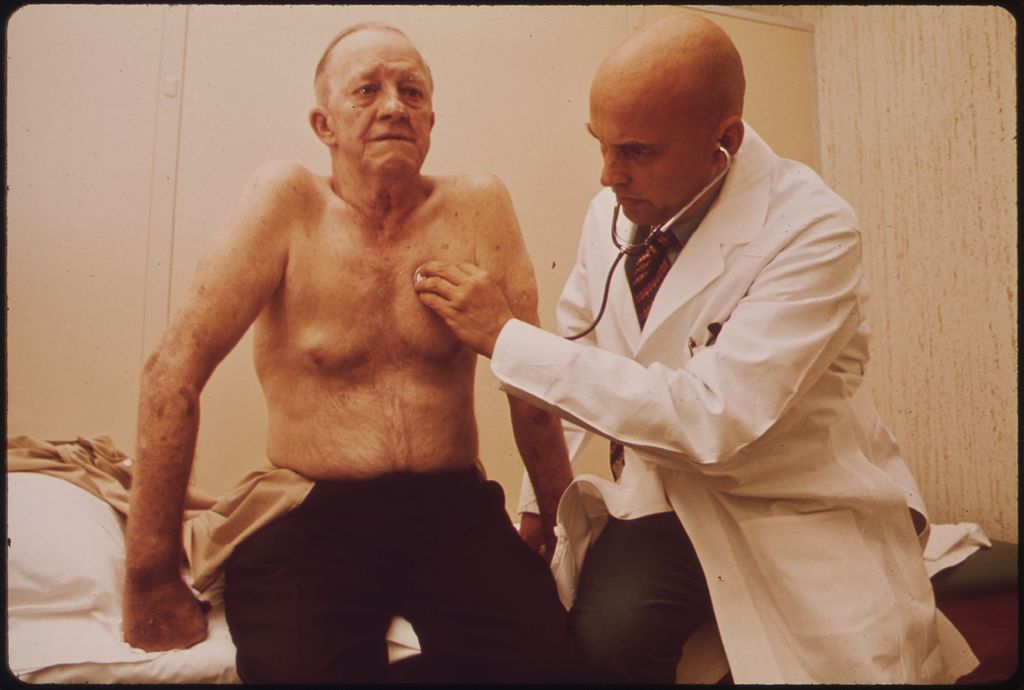
EMTs and Paramedics will routinely have to listen to and identify lung sounds. A good stethoscope is all that’s required, and the sounds heard during patient assessment can give critical clues about what’s happening during a respiratory emergency.
The video below demonstrates proper lung sound assessment technique — including patient positioning, stethoscope placement, and what to listen for:
Video: “The Lung and Thorax Exam” by BilderbackHealth via YouTube
Video: “Breath Sound - Bronchial vs Vesicular” by Drparth2008 via YouTube
Clear lung sounds are normal. This is what a patient should sound like during inspiration and exhalation when breathing normally. Clear, equal bilateral breath sounds on assessment means the airways are open and air is moving freely through all lung fields.
Video: “10 hours of Nothing” by e7magic via YouTube
Absent lung sounds are exactly what they sound like — nothing. There is no air moving through the bronchioles and no gas exchange occurring in the alveoli.
Diminished lung sounds are quieter than normal — air movement is reduced but not absent. They can occur in one lung or both.
Common causes include:
Unilateral diminished sounds (one side only) are a red flag — especially in a trauma patient where pneumothorax or hemothorax must be ruled out.
Video: “Breath Sounds - Wheezes” by Drparth2008 via YouTube
Wheezing is a high-pitched musical sound, usually heard on exhalation, caused by air being forced through narrowed airways. It is one of the most common lung sounds encountered in EMS.
Common causes include asthma, COPD, bronchitis, and allergic reactions.
Treatment:
Video: “Breath Sounds - Rhonchi” by Drparth2008 via YouTube
Rhonchi is characterized by a low-pitched, snoring-like sound caused by secretions or obstructions in the upper and larger airways. It is typically heard during both inspiration and expiration.
Common causes include pneumonia, chronic bronchitis, cystic fibrosis, and COPD. A key distinguishing feature: rhonchi may partially clear with coughing — this indicates the secretions are mobile in the larger airways, unlike crackles which do not clear.
Treatment: Supplemental O₂. Paramedic-level care may include bronchodilators and airway suctioning if the patient cannot clear secretions effectively.
Video: “Breath Sounds - Crackles” by Drparth2008 via YouTube
Crackles — also called rales — are caused by the explosive opening of small airways that have been collapsed or filled with fluid. They are more common during inspiration but can also be heard on expiration. Crackles are often associated with inflammation or infection of the small bronchi, bronchioles, and alveoli.
Fine crackles are soft, high-pitched, and brief — often described as the sound of opening a Velcro fastener or rolling a strand of hair between your fingers. They typically indicate pulmonary fibrosis or congestive heart failure.
Coarse crackles are louder, lower-pitched, and last longer than fine crackles. Their presence usually indicates an airway disease such as bronchiectasis.
Video: “Breath Sounds - Pleural Friction Rub” by Drparth2008 via YouTube
A pleural rub (friction rub) occurs when the lung is rubbing directly against the ribs. Normally, the pleural space between the lungs and chest wall is lubricated with fluid allowing frictionless movement. When this space is disrupted, a rough rubbing or creaking sound is produced during both inhalation and exhalation.
Common causes include pleuritis (pleurisy), pneumonia, and pulmonary embolism. The sound is often described as the sound of walking on fresh snow — a creaking, grating quality that is distinct from crackles.
Video: “Inspiratory Stridor” by logidragon via YouTube
Stridor is a high-pitched, almost whistling sound associated with narrowing of the upper airway. Unlike most lung sounds, stridor is often audible without a stethoscope. It can be inspiratory, expiratory, or biphasic:
Stridor is especially common in children with croup or epiglottitis.
| Sound | Quality | Phase | Common Causes |
|---|---|---|---|
| Normal | Clear, equal bilateral | Insp + Exp | Healthy lungs |
| Absent | Silent | — | Respiratory arrest, complete obstruction |
| Diminished | Quieter than normal | Insp + Exp | Pneumothorax, hemothorax, pleural effusion |
| Wheezing | High-pitched, musical | Mostly Exp | Asthma, COPD, bronchospasm |
| Rhonchi | Low-pitched, snoring | Insp + Exp | Secretions in large airways, pneumonia |
| Crackles | Popping/crackling | Mostly Insp | Fluid in small airways, pulmonary edema, CHF |
| Pleural Rub | Rubbing/creaking | Insp + Exp | Pleurisy, pulmonary embolism |
| Stridor | High-pitched whistle | Mostly Insp | Upper airway obstruction, croup |
Recognizing lung sounds quickly and accurately can change your field treatment decisions. Practice regularly with a quality stethoscope — the more patients you assess, the more natural pattern recognition becomes.
This guide is meant to supplement, not replace, your classroom instruction. Always follow your local protocols when treating respiratory emergencies.
For more on assessment tools, check out our guide to the best stethoscopes for EMTs and paramedics.
Test your understanding of clinical lung sounds, pathophysiology, and field treatments with this interactive 5-question NREMT-style quiz.
You are assessing a 6-year-old male presenting with respiratory distress. Even without a stethoscope, you hear a loud, high-pitched whistling sound during inspiration. What is this sound, and what does it suggest?
The 8 most important lung sounds are normal (clear), absent, diminished, wheezing, rhonchi, crackles (rales), pleural rub, and stridor. Each indicates a different underlying condition and guides your treatment decisions in the field.
Wheezing is a high-pitched sound on exhalation caused by narrowed airways. It is commonly associated with asthma, COPD, bronchitis, and allergic reactions. Treatment typically involves bronchodilators like albuterol for paramedics, and O₂ plus inhaler assistance for basic EMTs.
Rhonchi are low-pitched, snoring-type sounds caused by secretions in larger airways and may partially clear with coughing. Crackles (rales) are popping or crackling sounds caused by the explosive opening of small airways and often indicate pulmonary edema or fluid in the alveoli from heart failure.
Stridor is a high-pitched sound indicating upper airway obstruction. It is common in children with croup and is a medical emergency. Assess for visible foreign bodies, monitor the airway closely, and be prepared to intervene per local protocol.
Absent lung sounds mean no air movement is detected in the lungs. This indicates respiratory arrest or complete obstruction and requires immediate BVM ventilation. Paramedics should consider endotracheal intubation or a supraglottic airway device.
Use a quality stethoscope and compare bilateral lung fields — upper lobes anteriorly, lower lobes posteriorly, and lateral fields at the mid-axillary line. Ask the patient to breathe deeply through an open mouth and listen through both inspiration and expiration at each location.
About the Author
Veteran EMT with 13+ years of field experience in EMS. I built EMT Training Station to give aspiring first responders the honest, practical information I wish I'd had when starting out — covering training, certification, gear, and career advancement.
Learn how to become a flight paramedic. Read this step-by-step career roadmap covering clinical requirements, critical care certifications, and physical standards.
A veteran responder's guide to writing an EMS resume and passing the oral interview. Includes resume templates, certification checklists, and practice questions.
Learn how to become a firefighter EMT. Read this step-by-step career track guide covering EMT certification, CPAT fitness testing, and fire academy prep.